COVID
| Entry Date | Categories | Title | Content | hf:doc_categories |
|---|---|---|---|---|
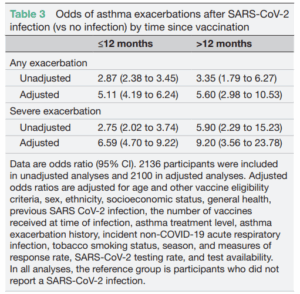
| December 16, 2025 | COVID | COVID-19 increases the risk of asthma exacerbation – UK study (2020-21) | A UK prospective study (conducted in 2020-2021) including 2100 people with asthma (that had had a vaccine booster in the past) reported that getting a COVID-19 infection increased the risk of asthma exacerbation by:
This study indicates that having a COVID infection continues to increase the risk of asthma flare-up in people with asthma, independently of asthma severity and asthma exacerbation history. While the results suggest that longer time since vaccination increases the risk of severe asthma exacerbation, the difference was not statistically significant (confidence intervals overlap) and this requires further investigation.
| covid viral-infections |
| July 28, 2023 | COVID | Experiences of Australians throughout the COVID-19 pandemic (Lung Foundation, 2022) – Resource | Report/Information paper by the Lung Foundation that discusses the results from their national survey (2196 responses) about the experiences of Australians throughout the COVID-19 pandemic and the impact of ongoing COVID-19 symptoms, particularly for the lung disease community. This report outlines the following: | covid viral-infections |
| July 20, 2022 | COVID, Emergency Department Presentations, Hospitalisation | Effect of COVID on asthma – AIHW | Extract from AIHW Chronic respiratory conditions report:COVID‑19 impact on chronic respiratory conditionsThe COVID‑19 pandemic had substantial impacts on hospital activity generally. The range of social, economic, business and travel restrictions, including restrictions on, or suspension of, some hospital services, and associated measures in other healthcare services to support physical distancing in Australia, resulted in an overall decrease in hospital activity between 2019–20 and 2020–21. As a result, the hospitalisation rates for asthma and COPD in these years were the lowest recorded in the last 10 years (AIHW 2022a). For more information on how the pandemic has affected the population’s health in the context of longer-term trends, see ‘Changes in the health of Australians during the COVID‑19 period’ in Australia’s health 2022: data insights. Emergency department presentations for asthma and COPD were also affected by the pandemic, decreasing from March (when the national lockdown started) to May 2020 (from 26 to 11 and 39 to 28 presentations per 100,000 population, respectively). In June 2020, emergency department presentations increased again as restrictions began to ease across the country (to 19 presentations per 100,000 population for asthma and to 33 presentations per 100,000 population for COPD) (Figure 9).
During the COVID‑19 pandemic (as at 31 October 2022), chronic respiratory conditions were certified as a pre-existing condition in 18% of the deaths with a chronic condition mentioned, the third highest of all chronic conditions (ABS 2022) Death rates due to all respiratory diseases combined also showed a substantial fall in 2020, with rates particularly low for females and during the winter months compared with previous years, though rates have increased since (Figure 10). While the long-term impact of COVID‑19 on the respiratory system is still being assessed, evidence shows that COVID‑19 does not directly impact the risk of increasing asthma severity and vice versa (Lee et al. 2020; Lieberman-Cribbin et al. 2020; Mather et al. 2021). However, there is increasing evidence showing that COPD patients with COVID‑19 have greater risk of mortality, severity of infection and higher likelihood of requiring Intensive Care Unit (ICU) support than those without COPD (Cazzola et al. 2021; Clark et al. 2021; Wells 2021). For more information, see ‘The impact of a new disease: COVID‑19 from 2020, 2021 and into 2022’ in Australia’s health 2022: data insights. | covid emergency-department-ed-presentations hospitalisation viral-infections |
| May 19, 2022 | COVID | Key guidelines for COVID and asthma – Resources | Key Guidelines: Infographics can be accessed here: https://toolkit.severeasthma.org.au/resources/infographics/ | covid viral-infections |
| May 19, 2022 | COVID | Key messages about asthma and COVID | key messages: | covid viral-infections |
| April 13, 2022 | COVID | COVID hospitalisation among people with asthma, multiple sources | HOSPITALISATION: – in a Scottish study, children aged 5-17 years with uncontrolled asthma (defined as hospital admission or oral corticosteroids prescription in the last 2 years) had at increased risk of hospital admission for COVID, with a risk increased by at least 6-fold for those with a history of asthma hospitalisation, and at leat 3-fold for those with a history of at least 2 courses of OCS in the last 2 years. The rate of hospitalisation was higher in children with poorly controlled asthma compared to those with well-controled asthma or no asthma.(2) – in a large national cohort study in England in adults and children aged 12-17 years old:(3) | covid viral-infections |
| April 13, 2022 | COVID | COVID deaths among people with asthma, multiple sources | MORTALITY: – In a large national cohort study in England:(4) | covid viral-infections |
| February 4, 2022 | COVID | Critical care hospitalisation for COVID among people with asthma, multiple sources | CRITICAL CARE: in hospitalised (severe COVID) patients: (1) | covid viral-infections |
| October 29, 2021 | COVID | Risk of COVID among people with asthma, multiples sources | – It was estimated that about 8% of adult COVID-positive patients have asthma1 | covid viral-infections |
| October 29, 2021 | COVID | GINA International guidelines recommendations for asthma and COVID | GINA International guidelines recommendations1: | covid viral-infections |
| September 21, 2021 | COVID | Urgent care in mild COVID patients, Randomised Controlled Trials Budesonide vs Usual Care: | URGENT CARE In mild COVID patients, Randomised Controlled Trials Budesonide vs Usual Care: | covid viral-infections |
| September 21, 2021 | COVID | Recovery in mild COVID patients,Randomised Controlled Trials Budesonide vs Usual Care : | RECOVERY in mild COVID patients,Randomised Controlled Trials Budesonide vs Usual Care : | covid viral-infections |